A short historical introduction:
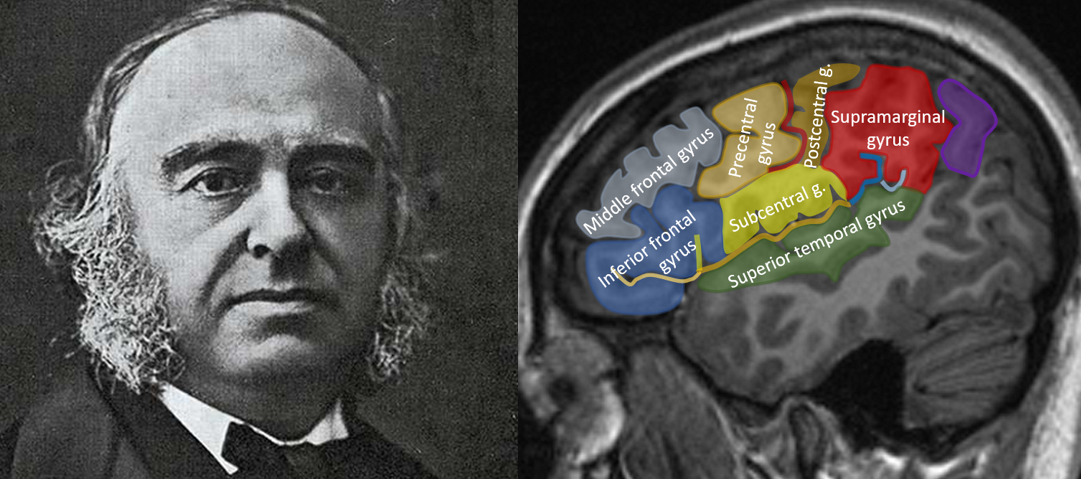
In 1861 the French physician Pierre Paul Broca performed an autopsy of the brain of a monsieur Lebornge. Monsieur Leborgne was a patient at the hospital where Pierre Paul Broca worked and had been suffering from loss of speech and right-sided paralysis for over 20 years. When mr. Leborgne died, Paul Broca examined his brain and discovered that the patient had a large defect posteriorly in the third frontal convolution (the inferior frontal gyrus) of the left hemisphere, probably the result of a stroke. Subsequently, Broca examined the brain’s off 11 other patients with similar loss of speech, found similar defects, and concluded that speech is a localized function in the human brain and resides posteriorly in the third frontal convolution of the left hemisphere. In 1909 Korbinian Brodmann published his maps on the cytoarchitectural organization of the human brain and since then the Broca area got defined in term of the “pars opercularis” and the “pars triangularis” of the inferior frontal gyrus, corresponding to Brodmann 44 and 45 respectively, of the dominant hemisphere.
What’s the dominant hemisphere?
The Broca area resides in the “dominant hemisphere”. The dominant hemisphere is the hemisphere where language functions reside. For most people, that’s the left hemisphere, but in about 4% of the population, language functions are localized in the right hemisphere. That number is even higher in left-handed people, and the right hemisphere is the dominant hemisphere in almost 30% of left-handed individuals. Still, that means even in left-handed individuals the left hemisphere is the dominant hemisphere in the majority of cases, so all in all, for most people, language functions (and the Broca region) are located in the left hemisphere.
How to find the inferior frontal gyrus on imaging?
The Broca area is not that hard to find on brain imaging. First we need to find the inferior frontal gyrus. That’s easiest to do in the sagittal plane. The inferior frontal gyrus is the lowest frontal gyrus on the lateral surface of the brain and often has a very characteristic M-shape, so just look for the lowest frontal gyrus shaped like an M. Like here:

Et voilà (as Broca would say), you’ve found the inferior frontal gyrus! The sulcus immediately above the inferior frontal gyrus is the inferior frontal sulcus, and the gyrus above that is the middle frontal gyrus. Easy no? Because it’s so easy, I immediately added the other perisylvian gyri for you on the second image. Immediately posteriorly of the middle and inferior frontal gyrus, we found the precentral gyrus (which makes sense when you think of it: speaking is a motor act, so for language to come out, we need our primary motor cortex), and behind that the postcentral gyrus. The precentral gyrus and the postcentral gyrus are united inferiorly in the “subcentral gyrus”.

Where’s the Broca area?
Now which part of the (dominant) inferior frontal gyrus contains the Broca area? The inferior frontal gyrus consists of three parts: the pars orbitalis (nearest to the orbit), the pars triangularis (the triangular shaped part in the middle), and the pars opercularis (the most posterior part, overlying the insula). These three parts are separated by small sulci, which are direct extensions of the Sylvian fissure. We’ve seen that Broca’s area corresponds to Brodman area 44 and 45, and that Brodman area 44 and 45 correspond to the triangular and opercular part of the inferior frontal gyrus, respectively. If we now try to identify the Broca area on imaging, we’ll find it in the middle and the posterior limb of the M-shaped inferior frontal gyrus.

Clinical significance?
Insults to the Broca area, mostly ischemic strokes, can lead to “Broca aphasia”. An aphasia is a disturbance in the production and/or comprehension of language. Broca aphasia, also known as expressive aphasia or motor aphasia, is a form of aphasia in which the speech production of a patient is disturbed (but speech comprehension is generally intact). Patients with Broca aphasia generally have a non-fluent, halting and effortfull speech. Patients may be able to produce some important “content words”, but leave out a lot of “function words” (words which have no meaning on their own, but an important grammatical function, such as prepositions and articles). This type of speech is also known as “telegrahic speech”. In very severe forms of Broca aphasia, patients can only utter single words, or may not be able to speak at all. Mr. Leborgne for instance was also known as “Mr. Tan”, because “tan” was the only word he could still produce.
Some critical remarks:
The classical 19th century model of language introduced by Broca, Wernicke and their contemporaries, in which language production is located in the Broca area and language comprehension in the Wernicke area (posteriorly in the superior temporal gyrus) relies on a very simplistic model of language. From a psychological point of view however, language is a lot more complex than just “lanague production” and “language comprehension”.
Furthermore, the Broca-Wernicke model is based on autopsy-studies, generally in a limited number of patients. In the case of Broca’s original study, Broca didn’t even perform a detailled examination of the brain of mr. Leborgne. He only observed a macroscopic defect in the left inferior frontal gyrus and concluded that his had to be the seat of language production. More than 100 years after Broca’s initial description, the brain of mr. Leborne (which is preserved and can still be admired) was re-examined with MRI. This MRI-study revealed that the damage in the brain of mr. Leborgne was a lot more extensive than the damage initially described by Broca.
There’s also the question of recovery. A lot of patients with an acute ischemic stroke in the anatomical Broca area present with a Broca aphasia in the acute phase, but may show extensive functional recovery following the insult despite having irreversible damage to the Broca area. This also suggests that the Broca area is probably not solely responsible for the complex processs of language production.
This was a lot of background information just to be able to recognize the Broca area on imaging, but I love this stuff and hope you found it as interesting as I do. If you have any questions or remarks, just post a comment! For those who are interested in the MRI-study on the brain of Mr. Leborgne, here’s a link to the article:
https://academic.oup.com/brain/article/130/5/1432/283170?login=false
Reference: Dronkers NF, Plaisant O, Iba-Zizen MT, Cabanis EA. Paul Broca’s historic cases: high resolution MR imaging of the brains of Leborgne and Lelong. Brain. 2007 May;130(Pt 5):1432-41. doi: 10.1093/brain/awm042. Epub 2007 Apr 2. PMID: 17405763.
Hi
I am Hassan Alturaiki, a 5th year medical student. I want to volunteer and help in this great work “the neuroradiologist”. I am a graphic designer also.